The HFEA's monthly newsletter for clinic staff |
| |
|
Upcoming deadlines for stored gametes and embryos |
On 31 December 2024 there are two important legal deadlines relating to the storage of gametes and embryos - appropriate actions must be taken where needed.
For further information, please refer to the October 2024 Clinic Focus. |
Update on PRISM and 10 Family Limit Alerts |
It is the clinic’s responsibility to ensure no donor breaches the 10 family limit in the UK, and clinics must follow Code of Practice guidance. We have however looked at ways we can provide information to help clinics with this. PRISM now allows us to execute new data interrogations upon the HFEA Register, and we have been carrying out testing of this process. Further to the letter shared with PRs in November, we plan to start sending automatic 10 Family Limit Alerts from 2 December 2024.
Thank you to the clinics who have already provided us with nominated email addresses for these new alerts to be sent to. If you haven’t yet, please send this information to register@hfea.gov.uk. How the 10 Family Limit Alerts will work
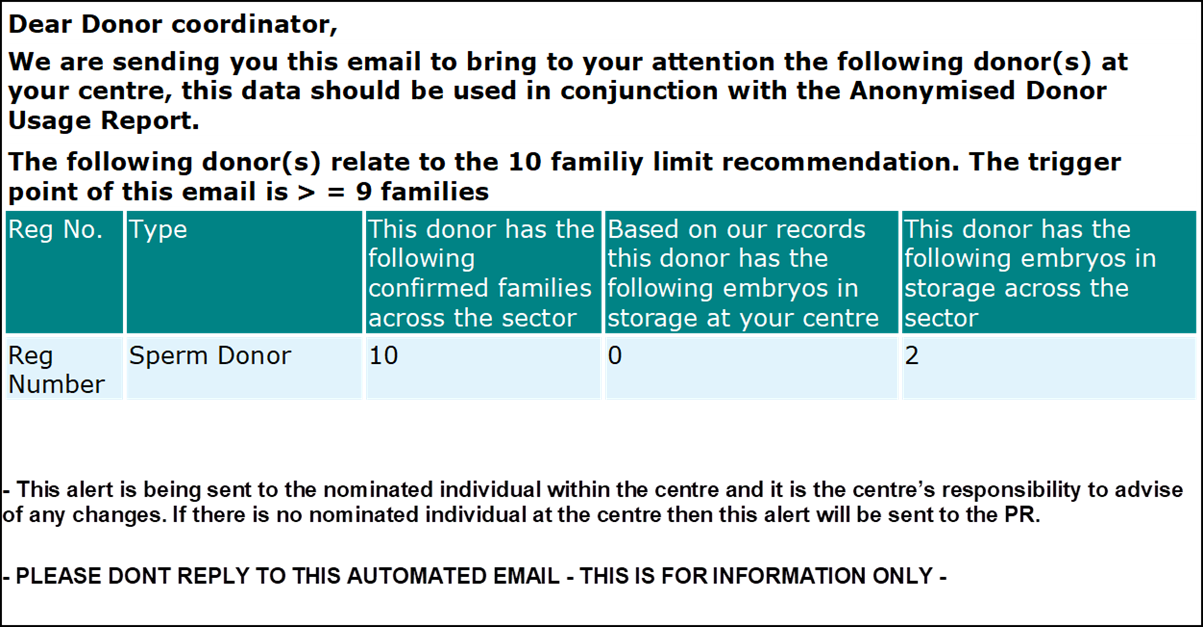
10 Family Limit Alerts will be sent on the morning after any data is received into PRISM which causes the alert to be triggered. This alert will be sent to the centre’s nominated individual if they reach nine or more families across UK licensed clinics, any subsequent activity thereafter which further changes the family count for this donor, or if the centre registers a donor which already has nine or more families elsewhere. An example of a 10 Family Limit alert is shown below: |
We define the family count within PRISM as including all cycles where a pregnancy or live birth has been reported, a lost to follow up, or we are awaiting early outcomes. We have observed that sometimes this means that the family count for a donor does go down as well as up. When this happens, recipients will be able to infer this from the alert report.
This alert system does not replace the internal alerts that clinics should have in place for when a donor has reached 6 families, as described in paragraph 11.63 of the HFEA Code of Practice.
In addition, we have also provided a report in PRISM that lists all the donors registered at the centre that currently have nine or more families. We hope this supports clinics in their awareness of all donors at their centre which might have been subject to previous alerts (had this process been running at the time), and against which, any subsequent alert received will be an incrementation to that list. We recommend that clinics take some time to familiarise themselves with this list ahead of receiving any new alerts. This report is entitled ‘donor family count >=9’ and can be found in the registration category of the reports section in PRISM. If you have any queries about 10 Family Limit alerts, please contact register@hfea.gov.uk.
New Donor Usage Report in PRISM
We would also like to signpost clinics to the new anonymised donor usage report in PRISM (again please reference the registration category in the reports section of PRISM).
This allows clinic or sperm bank staff to see all the instances where a specified donor has been used and across the sector and families to which they have contributed. This data is based on a unique identifier allocated to donors when they are registered with the HFEA, which means that if a donor is registered at more than one centre under different codes then all the outcomes will still appear. The old report will be retired in the next couple of months so we ask that clinic staff take the time to familiarise themselves with this new report. If clinic staff have any queries on this report, please contact register@hfea.gov.uk.
Please note this is providing extra mechanisms to check and be alerted to 10 family limits and centres must still follow Code of Practice Guidance. This includes the six family alert set out in 11.63 where the primary centre should notify any secondary centre within two working days. |
New NHS approach to patient safety incidents |
The HFEA has been discussing with NHS England how the new NHS approach to patient safety incidents will work with the statutory incident reporting requirements set out in the Human Fertilisation and Embryology Act and in the HFEA Code of Practice.
We have discussed some of the concerns clinics have raised with us regarding incident reporting requirements. The points below should clarify what these incident reporting requirements are. It is important to be clear that NHS England does not have mandatory reporting requirements, but contractually you must be able to report or have the ability to report. This should also be clear in your contracts. We hope the points below will help you to understand those reporting requirements. -
The Patient Safety Incident Response Framework (PSIRF) is the NHS’s new approach to responding to patient safety incidents. It replaces the previous Serious Incident Framework (SIF) and focuses on learning and improving patient safety. PSIRF emphasizes compassionate engagement, system-based learning, proportionate responses, and supportive oversight.
- NHS England patient safety incident reporting system has been updated from the NRLS (the National Reporting and Learning System) to the learn from patient safety events service (LFPSE). When reporting incidents via a Trust’s Local Risk Management System (LRMS e.g. Datix, Ulysses or Sentinel) instead of having to submit manually the data to the NRLS, LFPSE supports real-time, automated uploading.
-
For smaller NHS care providers e.g. IVF clinics providing care for NHS patients via local commissioning bodies NHS England does not have mandatory reporting requirements, but contractually, all NHS providers working under the NHS Standard Contract must be
able to report either by their own system e.g. Datix that is connected to LFPSE or via a direct log into the online LFPSE portal. Contracts clearly state that they must be
able to report, the option is given in case incident reporting via eg Datix is perceived to be a punishment and hence a barrier to reporting patient safety incidents.
- This information is captured to learn from patient safety incidents, and it is not for the patient safety events service to investigate the reported incidents.
-
Statutory legislation remains in place e.g. centres must report incidents to the HFEA via the incident reporting system. In the same way a safeguarding concern/issue must be reported to the CQC, abuse or alleged abuse involving a person(s) using the service, whether the person(s) are the victim(s), the abuser(s), or both. This is no change to the current process.
-
RCA methodology is often seen as too narrow/reductive and linear – PSIRF (Patient Safety Incident Response Framework) reflects the need and appetite to broaden out the investigation scope to capture more nuanced information to enhance and improve patient safety.
-
The SEIPS (Systems Engineering Initiative for Patient Safety (SEIPS) framework is a human factors-based approach used to understand outcomes within complex socio-technical systems, such as healthcare1. It acknowledges that healthcare is both highly variable and dynamic, and it characterizes it as a socio-technical system with multiple interactions between human and technological components.
HFEA incident reporting requirements are set out here and further information can be found in the Code of Practice.
|
‘Family formations in fertility treatment 2022’ report published |
This week we published our ‘Family formations in fertility treatment report 2022’.
Key findings from the report include: - Female same-sex couples had the highest birth rate among all family types
-
One in six of all IVF and DI treatments were had by female same-sex couples or single patients.
- Opposite-sex couples were three times as likely to receive NHS funding than single patients and female same-sex couples.
The data shows that most fertility treatments in the UK were among opposite-sex couples (89%). However, there has been a notable increase in the number of single patients (6%) and female same-sex couples (4%) having fertility treatment.
From 2012-2022, the number of patients having IVF or DI treatment increased from around 45,300 to 47,000 for opposite-sex couples, 1,300 to 3,300 for female same-sex couples and 1,400 to 4,800 for single patients.
Overall, surrogacy cycles accounted for 0.4% of all IVF treatments in 2022, with the number of surrogacy patients increasing from 130 in 2012 to 230 in 2022.
Our report also found the age at starting treatment varied in each group. Single patients were the oldest group, though their average age when starting IVF treatment decreased the most, from almost 38 years old (37.9) to just over 36 years old (36.4) – the youngest since data collection began in 2008. From 2018-2022, egg freezing was highest among single patients, making up 89% of all egg freezing cycles. However, more opposite-sex couples thawed eggs for treatment (85%), followed by single patients (13%) and female same-sex couples (2%). Although many more female same-sex couples and single patients are having fertility treatment, both groups were less likely than opposite-sex couples to receive NHS funding. About 16% of female same-sex couples and 18% of single patients had NHS funding for their first IVF treatment compared to 52% of opposite-sex couples aged 18-39.
You can read the full 'Family formations in fertility treatment 2022' report here. Our HFEA dashboard, which allows users to explore HFEA data and find statistics on their own areas of interest, has also been updated.
|
New members appointed to the HFEA Authority |
In October four new members were appointed to the HFEA Authority (Board) by the Secretary of State for Health and Social Care. The new members will play a key role in the effective governance of the HFEA, and help retain public and professional confidence in the regulation of fertility treatment and embryo research in the UK.
Tom Fowler, Deputy National Director of Health Protection and Screening Services at Public Health Wales, Rosamund Scott, Professor of Medical Law and Ethics and Director of the Centre of Medical Law and Ethics at King’s College London, Anya Sizer, freelance fertility consultant and Trustee of Fertility Alliance, and Stephen Troup, consultant reproductive scientist and Founder Member of the Association of Reproductive and Clinical Scientists (ARCS), began their three-year term in October 2024.
To find out more about the HFEA’s Authority members, click here. |
New guidance on changes to the law on screening for reciprocal IVF and known donors with undetectable HIV |
Reciprocal IVF (partner to partner donation)
Same-sex couples having reciprocal IVF should undergo the same screening carried out before treatment as heterosexual couples providing their own gametes for IVF.
We have new information for patients about reciprocal IVF on the HFEA website. Known donation from individuals with undetectable HIV
This change in the law allows known donation from individuals living with HIV with an undetectable viral load (including intended parents providing eggs or sperm as part of a surrogacy arrangement). It will not affect gamete or embryo donors in general, who will still be required to be negative for HIV1 and 2.
In order to implement the new HIV screening requirements, clinics must have the conditions on their licence amended to reflect the new law. The October 2024 special edition of Clinic Focus outlines the process for updating licences and guidance to support you to implement these changes.
If you have any questions, please contact your HFEA Inspector. |
October 2024 Scientific and Clinical Advances Advisory Committee (SCAAC) minutes available |
Minutes from the SCAAC meeting held on the 7 October 2024 are now available on the SCAAC webpage.
The Committee was joined by the team at Newcastle Fertility Centre who presented on the progress of the Mitochondrial Donation Programme. This was followed by discussions on stem cell-based embryo models, in vitro derived gametes, and scientific considerations relevant to the 14-day rule. |
New venous thromboembolism (VTE) guidance published by the British Fertility Society |
The British Fertility Society (BFS) has published new guidance to help clinics prevent venous thromboembolism (VTE) in medically assisted reproduction (MAR). While VTE is a recognized complication of MAR, it is largely preventable with appropriate care. The aim of this guidance is to provide clinicians with clear information on VTE risk factors, practical tools for assessing risk, and best practice recommendations for reducing risks in those undergoing MAR treatments.
Clinics are encouraged to review the full document, which includes a VTE risk assessment tool in Appendix A and prophylaxis guidance based on risk classification in Appendix B, now available here. |
-
Alert 2024/17 – Field Safety Notice: [Update to Ultragel Medical Kft, AquaUltra Clear Ultrasound Transmission Gel]
Alert 2024/17 was issued on 12 November 2024
If the PR at your clinic did not receive this alert via email, please contact Business Support at HFEACompliance@HFEA.gov.uk to update your contact details. Please also make sure that the email address alerts are sent from, alert@hfea.gov.uk, has been whitelisted by your IT department. For any questions about the content of the Alerts, please contact incident.reporting@hfea.gov.uk. |
|
|
Regarding imports from third country suppliers (TCS)*
When applying for authorisation to import multiple samples from a TCS, you may be asked to provide the most up-to date version of a number of documents with the application, as per ‘Information tool B’ Regulatory changes to imports and the ITE import certification scheme from 11pm on 31 December 2020 and 11pm on 30 June 2021.
Import agreements with suppliers should be regularly reviewed and if necessary, revised to reflect any changes in the standards required by the Human Fertilisation and Embryology Act 1990. Please see audit tool A within the document linked above, which lists the clauses which must be included within your import agreement.
For multiple imports, the length of the authorisation will be tied to your centre’s licence length and will be renewed (without the requirement for re-application) as part of the licence renewal process. If inspections associated with the licence renewal find non-compliance in your centre’s import relationship with a third country supplier (TCS), the certificate may be revoked or suspended, in part or in full, depending on the non-compliance found.
Centres are also reminded that where special directions for imports are granted, an ITE is still required and should be applied for. *For centres in GB after 11pm on 30 June 2021, all countries outside of the United Kingdom (England, Scotland, Wales, and Northern Ireland) are third countries including those in the EEA and Gibraltar. For centres in NI after 11pm on 31 December 2020, all countries outside of the EEA, including GB and Gibraltar, are third countries. General direction 0006 |
|
|
Editorial statement
Clinic Focus is the official electronic newsletter of the Human Fertilisation and Embryology Authority, is produced by the editorial team of the HFEA and provides a monthly roundup of news and information for clinics and their staff working in the field of fertility treatment. No part of this publication may be reproduced without prior permission. You can view our privacy policy on our website. Click here to unsubscribe 2 Redman Place London E20 1JQ © Copyright Human Fertilisation and Embryology Authority, 2019 |
|
|
|